Overview
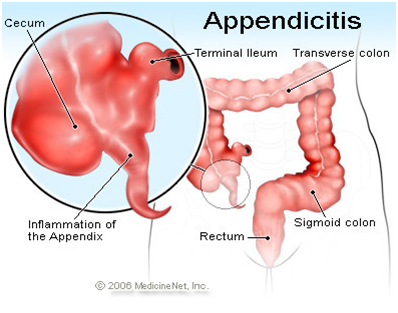
The appendix is a narrow tubular pouch attached to the intestines. When the appendix is blocked, it becomes inflamed and results in a condition termed appendicitis. If the blockage continues, the inflamed tissue becomes infected with bacteria and begins to die from a lack of blood supply, which finally results in the rupture of the appendix (perforated or ruptured appendix).
The American Journal of Epidemiology study found that appendicitis was a common condition affecting approximately 6.7% to 8.6% of the population. IN the U.S. 250,000 cases of appendicitis are reported annually. Individuals of any age may be affected, with the highest incidence occurring in the teens and twenties; however, rare cases of neonatal and prenatal appendicitis have been reported. Increased vigilance in recognizing and treating potential cases of appendicitis is critical in the very young and elderly, as this population has a higher rate of complications. Appendicitis is the most common pediatric condition requiring emergency abdominal surgery.
Appendicitis Causes
There is no clear cause of appendicitis. Fecal material is thought to be one possible cause of obstruction of the appendix. Bacteria, viruses, fungi, and parasites can result in infection, leading to the swelling of the tissues of the appendix wall. The various infecting organisms include Yersinia species, adenovirus, cytomegalovirus, actinomycosis, Mycobacteria species, Histoplasma species, Schistosoma species, pinworms, and Strongyloides stercoralis. Swelling of the tissue from inflammatory bowel disease such as Crohn's disease also may cause appendicitis. Appendicitis is not a hereditary disease and is not transmittable from person to person.
Appendicitis Symptoms and Signs
Appendicitis typically begins with a vague pain in the middle of the abdomen often near the navel or "belly button" (umbilicus). The pain slowly moves to the right lower abdomen (toward the right hip) over the next 24 hours. In the classic description, abdominal pain may be accompanied with nausea, vomiting, lack of appetite, and fever. All of these symptoms, however, occur in fewer than half of people who develop appendicitis. More commonly, people with appendicitis have any combination of these symptoms.
- Symptoms of appendicitis may take 4-48 hours to develop. During this time, a person developing appendicitis may have varying degrees of loss of appetite, vomiting, and abdominal pain. The person may have constipation or diarrhea, or there may be no change in bowel habits.
- Early symptoms are often hard to separate from other conditions including gastroenteritis (an inflammation of the stomach and intestines). Many people admitted to the hospital for suspected appendicitis leave the hospital with a diagnosis of gastroenteritis; initially, true appendicitis is often misdiagnosed as gastroenteritis.
- Children and the elderly often have fewer symptoms, or cannot adequately describe their symptoms, which makes their diagnosis less obvious and the incidence of complications more frequent.
Appendicitis Diagnosis
Appendicitis is diagnosed by the classic symptoms of appendicitis and physical examination (the health care practitioner's examination of the patient's abdomen).
- Lab work: Although no blood test can confirm appendicitis, a blood sample is sent for laboratory analysis to check the white blood cell count, which is typically elevated in an individual with appendicitis. However, normal levels can be present with appendicitis, and elevated levels can be seen with other conditions. A urinalysis may be ordered to exclude urinary tract infection (or pregnancy) as the cause of the patient's symptoms.
Imaging tests: Imaging tests are ordered when the diagnosis is not readily apparent. Most medical centers utilize a CT scan of the abdomen and pelvis to assist in evaluating abdominal pain suspected of
- being caused by appendicitis. Ultrasound scanning is commonly used in small children to test for appendicitis in order to avoid exposing the child to radiation from CT scans.
Other conditions that cause abdominal pain may mimic the symptoms of appendicitis making the diagnosis more difficult. These conditions include kidney stones, urinary tract infections, hernias, gallstones and gallbladder problems, colitis, diverticulitis, and ovarian or testicular problems
Surgery (Appendectomy)
The best treatment for appendicitis is surgery to remove the appendix (appendectomy) before the appendix ruptures. While awaiting surgery, the patient will be given IV fluids to keep well hydrated. The patient will not be allowed to eat or drink because doing so may cause complications with the anesthesia during surgery.
Surgery is commonly performed via laparoscopy, a minimally invasive procedure where small "keyhole" incisions are made in the abdomen and the appendix is removed with the assistance of a small camera guided by the surgeon. However, in some cases it may be necessary to do an open abdominal procedure to remove the appendix.
Occasionally, surgery for appendicitis reveals a non-inflamed appendix (negative appendectomy), with high rates in infants, the elderly, and young women. However, the use of imaging studies (CT scans, ultrasounds) appears to have reduced the negative appendectomy rate to 7%-12%. The difficulty in making a definite diagnosis of this medical problem and the risk of missing an acutely inflamed appendix (and the patient becoming very ill due to perforation) makes a certain rate of misdiagnosis inevitable. Women in particular have a high rate of negative appendectomy as ovarian and uterine problems make the diagnosis more difficult. CT scanning prior to surgery has been shown to decrease this percentage to closer to 7% to 8% in women. |