Introduction:
Laparoscopic cholecystectomy has replaced open cholecystectomy as the gold standard surgical procedure for majority of patients with gall stone disease1. Standard laparoscopic surgeries, such as laparoscopic cholecystectomy, are routinely performed using one 10 mm umbilical incision and three ancillary 5/10mm trochars placed over the anterior abdominal wall. Many laparoscopic surgeons have been attempting to reduce incisional morbidity and improve cosmetic outcomes by using fewer and smaller ports.1 With advances in endoscopic procedures and instrumentation, surgery has dramatically advanced from open procedures to "minimally invasive" surgeries. Surgeries that traditionally involved multiple trochars and multiple incisions have advanced to surgeries involving access through a single site, such as the umbilicus alone, with improved safety, cosmesis, lesser pain, decreased operative time, improved recovery, and at a lesser cost. 2 Single port surgeries ideally involve the use of a special port with 3 to 4 channels into which the trochars and instruments are passed into the peritoneal cavity through a single intraumbilical incision of 2 to 2.5 cm to perform the surgery.SILS is a rapidly evolving method that is complimenting traditional laparoscopy in selected cases. 4,5 This incision had disadvantages of possibility of an incisional hernia and led to the use of multiple port s in the same single intra umbilical incision thus eliminating the need to use any specialized expensive port. The use of only one intraumbilical 10mm-15mm incision offers all the benefits of minimally invasive surgery like minimal bleeding, less post operative pain, short hospital stay, early return to daily activity, less chance of wound infection and port site hernia, and a virtually invisible cosmetic scar. The surgery is performed with traditional straight laparoscopic instruments which are 45 cm long and a 30 degree 5 mm scope and 2 minilap verress needle instruments.
Operative procedure:
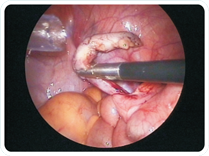
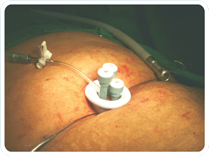
The patient is in a lithotomy position with the arms by the sides on the table. The surgeon stands between the legs of the patient, the assistant on the left of the patient and the staff nurse on the right of the patient. An intra-umbilical incision of 1.5 cm is used and a subcutaneous flap is raised. One 10 mm trocar and one 5 mm trocar is introduced in the incision pointing towards the gall bladder. A 5 mm high definition full screen scope is used for vision and the operating instruments are inserted through the 10 mm channel with the help of a 10 to 5 reducer. The fundus and hartmanns pouch of the gall bladder are retracted with the help of two sutures of 2-0 ethilon on straight needle introduced through the skin in the right hypochondrium, or introduction of two 2 mm verress needle minilaparoscopic instruments. The anterior and the posterior peritoneum are dissected with the help of the hook or Maryland forceps and monopolar cautery.The lymph node is identified and the cystic artery is dissected. The anterior and the posterior windows are made in the peritoneum and the cystic duct is completely dissected at the junction of the hartmanns pouch with the cystic duct. Clips are applied on the cystic duct and the cystic artery, two on the patient end and one on the specimen side after obtaining the triangle of safety. The duct and the artery are cut and with the help of the monopolar hook electrode, the gall bladder is dissected of the liver fossa. Haemostasis in this area is easily achieved with the use of a bipolar forceps. The traction on the gall bladder is periodically adjusted with the help of the minilap instruments. The separated gall bladder is then inserted in a sterile plastic bag. Saline wash is given and the fluid aspirated. If the gall bladder is distended with bile , it can be aspirated with a syringe and a needle after bringing it partially out through the umbilical incision. Alternatively the 10mm and the 5mm incisions can be combined to deliver the gall bladder. The incision can then be closed with non absorbable material to reduce the incidence of incisional hernia. The 2 mm minilap punctures do not need to be closed. Sub cuticular monocryl stitches are used for closure of the umbilical incision. The gall bladder is sent for histopathology.
Discussion:
Single port laparoscopic surgery where a specialized port was used had all the disadvantages of an expensive port and disposable roticulators, larger incision, increased post operative pain, seroma formation and wound infection and occurrence of incisional hernia. All these disadvantages have been nullified with the help of single incision multi trocar laparoscopic surgery. This procedure is highly cosmetic as none of the incisions are visible after a minimal healing period. Also return to normal activity is much faster compared to multi trocar conventional laparoscopic cholecystectomy. The known limitations include a higher learning curve for the surgeon, clashing of instruments, frequent re adjustments of the instruments and camera port for obtaining the critical view of the important structures, good co-ordination between the operating surgeon and the assistant as well as the second assistant and inability to operate on complicated cases of acute cholecystitis, perforation, gangrene or bowel adhesions. However, most of these limitations are subjective to the skill and experience of the surgeon, who with progressive practice and a little more perseverance can do seemingly impossible instrument maneuvers with ease. A careful selection of cases and technique will help the surgeon to offer progressive levels of minimally invasive surgery, ranging from (1) standard laparoscopic cholecystectomy where 4 incisions ( 10 mm x 1 intraumbilical incision and additional 3 incisions) are made over the anterior abdominal wall, to (2) SILS cholecystectomy - where a 2.5 cm umbilical incision is made into which special port having channels for 3 trochars are introduced, to (3)Single incision laparoscopic cholecystectomy – where only one 10 mm-15 mm incision is made in the umbilicus.
Conclusion:
This laparoscopic technique is simple to perform, easily reproducible, that can be performed with standard laparoscopic instruments and with many advantages as mentioned above. It offers an excellent alternative to the conventional multi-port, multichannel surgery in carefully selected patients, By employing a only a single incision, this technique helps to reduce the complications of multiple ports as in Standard Laparoscopic Surgery or that of large incision and port of SILS Technique. Single incision laparoscopic surgery for cholecystectomy appears to a feasible and promising method for treatment of symptomatic gall stones.6 This surgery can be performed safely with traditional laparoscopic instruments.7thus making key hole surgery a practical reality thereby offering the patient minimally invasive surgery in the true sense.
|