Surgical team
•Advanced Laparoscopic Team well versed with traditional laparoscopy.
•Accurate co ordination between surgeon and camera holder {constant team}
•Limited range of movement and clashing of instruments.—PATIENCE
•Counter intuitive movements.
•Hypo-tensive anaesthesia with good muscle relaxation.
Commonly performed procedures
•Cholecystectomy
•Appendicectomy
•Hysterectomy
•Salpingo-ophorectomy
•Diagnostic laparoscopy with biopsy
Urology and bariatric procedures
TECHNIQUE
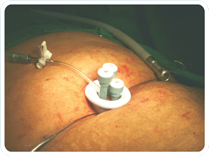
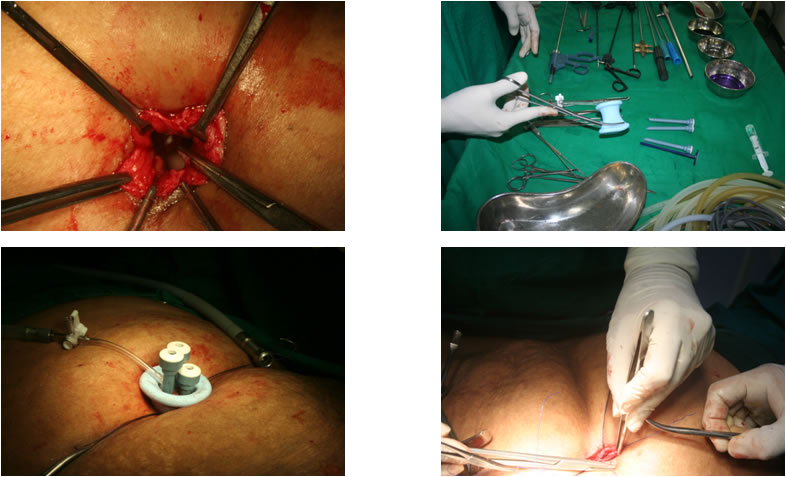
•2-2.5 cm incision in the umbilicus.
•Stay sutures taken on the sheath.
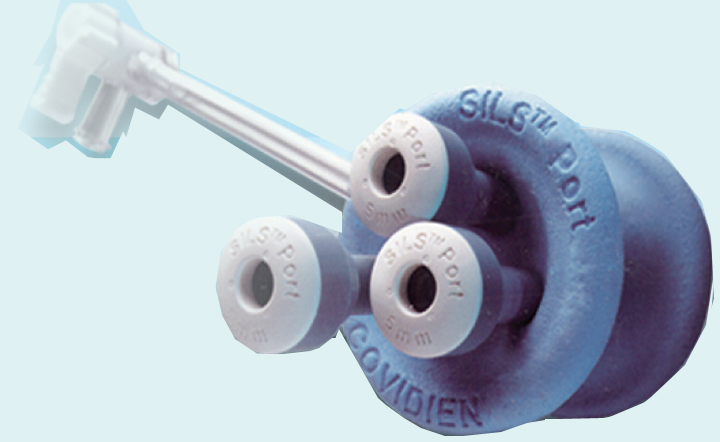
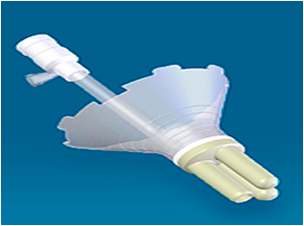
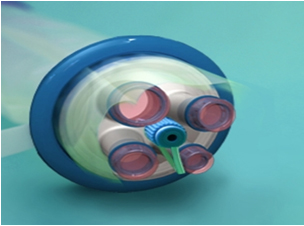
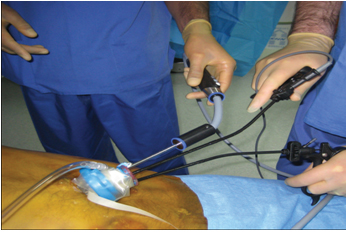
•SILS port held with introducer and thrust into the peritoneal cavity.
•5 mm cannulaes introduced into the port and insufflation started.
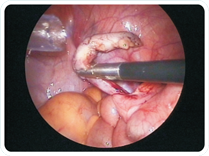
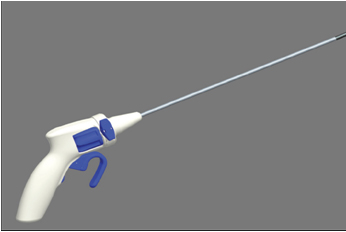
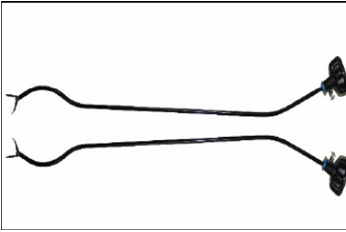
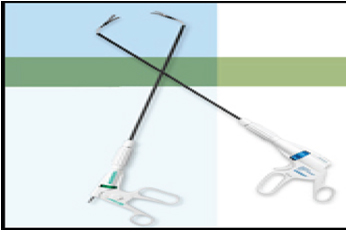
•Surgery carried out with routine straight laparoscopic instruments and roticulators.
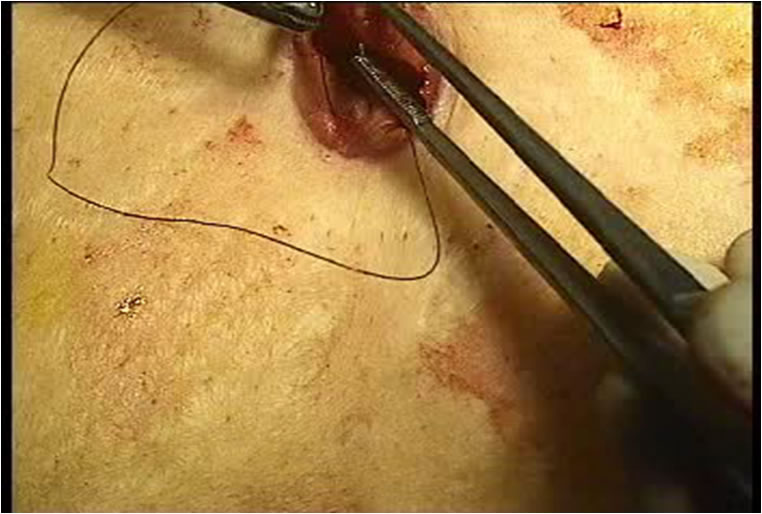
•Sheath closed with non absorbable 1-0 prolene stitches and subcuticular Monocryl to skin.
Advantages and Limitations
•PROPOSED ADVANTAGES
•Improved cosmesis
•Decreased post-operative pain
•Early return to activity |
•KNOWN LIMITATIONS
•Steep learning curve
•Cost of equipment
•? Long term complication of incisional hernia.
•Difficult in acute and inflammed organs. |
INSERTION OF PORT

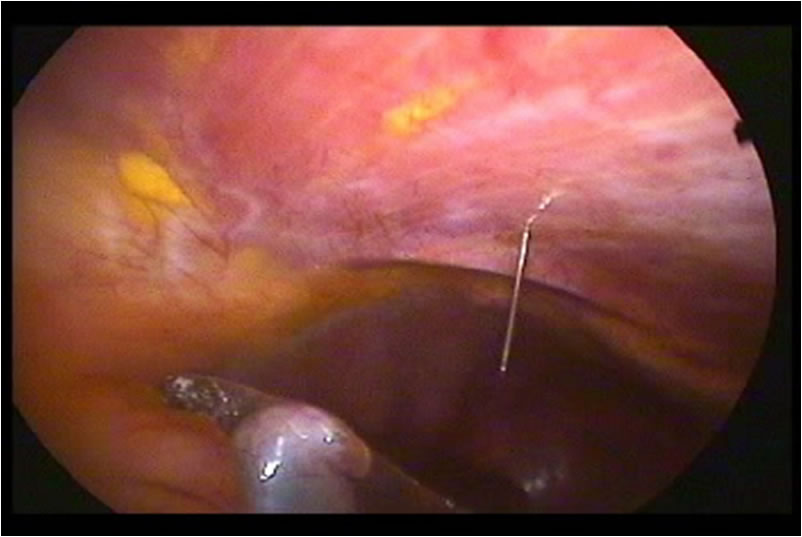
SILS APPENDICECTOMY

SILS HYSTERECTOMY
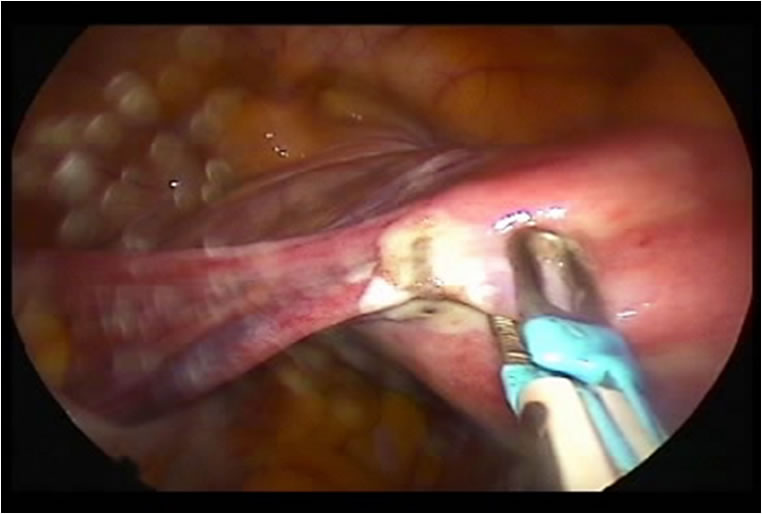
SILS CHOLECYSTECTOMY
CLOSURE OF INCISION
Discussion
 
•Any other advantage besides cosmeses??
•Cost of equipment
•Learning curve
•Safety Profile
Future of SILS
•Will depend on the following
1.Equipment cost
2.Social Acceptance
3.Surgeon skill
4.Training programmes
5.Instrument innovations
6.Professional enthusiasm
7.Mediclaim re-imbursements
OLD CONCEPT:
DO OR DIE
NEW CONCEPT:
DO IT BEFORE YOU DIE
LATEST CONCEPT:
DON’T DIE UNTIL YOU DO IT
Meanwhile The Future Is Here-SILS
Lets keep it this way


|