SINGLE TROCAR(10-MM) INCISION LAPAROSCOPIC APPENDECTOMY (STILS)
Abstract:
Single port surgery is an emerging advancement in the field of minimally invasive surgery .Refinement and modification of laparoscopic instrumentation has resulted in substantial increase in single port surgeries. The use of a single trans-umbilical incision affords maximum cosmetic benefit as the incision is completely hidden in the umbilicus. The advantages may be decreased pain, early mobility and a cosmetically acceptable scar, but there has been an increased concern of port site infection, seroma formation and hernia. To obviate these concerns we have developed a technique of STILS which is single trocar 10-mm incision laparoscopic surgery. We have performed hysterectomies, appendectomies, cholecystectomies, tubal ligations and unruptured ectopic surgeries with this technique. We have performed these surgeries with a 10-mm operating laparoscope having a 5-mm channel through which an instrument can be passed .We describe here a case of laparoscopic appendectomy by the STILS technique.
Introduction:
In recent years surgeons quest to reduce the size and number of incisions has lead to the development of several new innovations in the technique of surgery as well as instrumentation. Natural orifice trans-lumenal endoscopic surgery(NOTES) and single incision laparoscopic surgery(SILS) have been two such advances. Because of the potential hazard of trans-visceral access associated with (NOTES), greater interest has been generated for (SILS). There has not been widespread acceptance of (SILS) due to the fears of port site herniation and wound infection. This led to the development of single incision surgery without the use of the port. Multiple ports were used through the single trans-umbilical incision using conventional trocars and instruments thus decreasing the cost as well the possibility of port site herniation. We have modified this technique and have started doing surgeries through a single 10-mm incision in the umbilicus. The technique has been possible due to the use of a long term forgotten tool known as the operating laparoscope. This operating laparoscope is a 10-mm scope with a 5-mm channel for the passage of 45 cm long instruments. Multiple surgeries like appendectomy, cholecystectomy, hysterectomy, tubal ligation, diagnostic laparoscopy, lymph node biopsy, unruptured ectopic, TEPP, etc. can be performed with the help of this operating laparoscope with a single 10-mm incision in the umbilicus which is virtually invisible and carries almost negligible chances of wound infection and herniation. We report a case of single incision laparoscopic appendectomy by the STILS technique.
Instrumentation:
10-mm trocar, 45 cm hand instruments. (bipolar forceps, scissors, grasper and knot pusher,suction irrigation cannula)
Operative procedure:
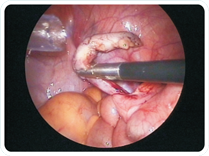
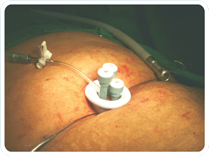
The surgery was carried out under general anaesthesia. Patient was placed in lithotomy position. The surgeon stood at the left side of the patient and the assistant stood in between the legs of the patient. The abdomen was prepared and draped. The verres needle was inserted in the umbilicus. After confirming the presence of the verres needle in the umbilicus,insufflation was started. After attainment of the set pressure, the 10-mm trocar was inserted in the umbilicus. Head low and right side up position was used. The 10-mm operative laparoscope was inserted in the trocar and a check scopy was done to see the feasibility of completion of surgery through a single trocar or the need for additional trocars like in a conventional laparoscopy. The appendix was visualized and grasped with a 5-mm grasper through the operating scope. A 1-mm grasping forceps introduced through the verres needle placed near the right anterior superior iliac spine was used to grasp the appendix. The bipolar forceps was used to burn the mesoappendix from the tip to the base. After the entire appendix was made bereft of the mesentry, a 0-no catgut endoloop was used to tie a knot at the base of the appendix after milking the faecolith. Another two endoloops were placed on the appendix. The appendix was cut with the scissor and the mucosa was cauterized with the bipolar forceps. The appendix was brought out through the operating laparoscope under direct vision. The rest of the bowel was explored. The scope and trocar were removed and the sheath was closed with 2-0 prolene and skin with 3-0 monocryl sutures. A single waterproof dressing was used at the umbilical site. The surgery was completed in 30 minutes with negligible blood loss.post-operative liquids were started on the same day within 6 hours and the patient was discharged after 24 hours. The patient was given a single shot of intra-venous antibiotic before the surgery and was discharged on oral antibiotics for 5 days at the time of discharge.
Discussion:
A traditional laparoscopic appendectomy involves three trocars,requiring three separate incisions. A10-mm umbilical port is placed and two 5-mm ports for retraction and dissection. In single port appendectomies using the available ports, a 2.5 cm incision is taken in the umbilicus and multiple instruments are inserted through the multiple channels in the same port.Various techniques have been described where surgeons have performed appendectomies without the port by insertion of a trocar in the umbilicus and using a transdermal suture to elevate the appendix for dissection and retraction.[1,2].The extracorporeal technique involves the insertion of one 10-mm trocar through the umbilicus and use of an 8m laparoscope with 5-mm operating channel. The appendix is brought out through the umbilicus and the appendix is divided extracorporeally.[3].Single port , transumbilical, extracorporeal appendectomies have been shown to be safe and effective alternatives to the traditional laparoscopic appendectomy with a comparable post operative complication rate.[4-11].Using an instrument which passes through the verres needle obviates the need of an other incision and also makes it possible to do difficult cases of adhesions, peritonitis or retrocaecal appendix.The surgeon is not dependent on an assistant to hold the camera and hence vision is not hampered during the surgery. The patient benefits from the decreased invasiveness of the surgery as well as the decreased cost as it does not involve any expensive port or special instruments like roticulators. Difficult cases can always be converted to traditional laparoscopic surgery by insertion of additional ports and completing the procedure. The only limitation to the technique is the learning curve which is common to any new technique. But even that is not very steep due to the sole reason that only one instrument is placed through the working port greatly improving the economy of motion. The post-operative pain is almost negligible and the patient does not require any analgesics on discharge. The scar, being completely hidden in the umbilicus gives the utmost cosmetic result which cannot be better than any other method of surgery for appendix. The operating laparoscope can prove to be the most important development in the advancement of single incision laparoscopic surgery, thus giving the patient the benefit of a true key hole surgery.
Conclusion:
Single trocar appendectomy is a cost effective procedure as it helps in decreasing the amount of equipment, operating room staff and operating room time required to complete the procedure. It is beneficial to the patient in the form of decreased post operative pain, improved cosmeses due to a virtually invisible scar and quicker recovery. It has been shown to be safe and effective and will some day replace traditional laparoscopy in the performance of minimally invasive operation.
|