SINGLE ( 10 mm ) TROCHAR- INCISION LAPAROSCOPIC HYSTERECTOMY
Introduction
Standard laparoscopic surgeries, such as laparoscopic hysterectomy, are routinely performed using one 10 mm umbilical incision and three ancillary 5/10mm trochars placed over the anterior abdominal wall. Many laparoscopic surgeons have been attempting to reduce incisional morbidity and improve cosmetic outcomes by using fewer and smaller ports.1 With advances in endoscopic procedures and instrumentation, surgery has dramatically advanced from open procedures to "minimally invasive" surgeries. Surgeries that traditionally involved multiple trocars and multiple incisions have advanced to surgeries involving access through a single site, such as the umbilicus alone, [laparoendoscopic single site surgery (LESS), single incision laparoscopic surgery (SILS), single-instrument port laparoscopic surgery (SIMPL)], with improved safety, cosmesis, lesser pain, decreased operative time, improved recovery, and at a lesser cost. 2 Single-incision surgeries ideally involve the use of a special port with 3 to 4 channels into which the trochars and instruments are passed into the peritoneal cavity through a through a single intraumbilical incision of 2 to 2.5 cm to perform the surgery.. Surgeries for which the LESS/SILS procedures have proven to be effective include cholecystectomy, hysterectomy, appendecectomy. Although SILS may be more accurate as an acronym, the term fails to recognize devices that allow multiple instruments through the same device.3 In our recently devised Single Incision- Single Trochar laparoscopic technique , described in the following sections, is an attempt to strictly adhere to the concept of single-site, single port sugery by using only one intraumbilical10 mm incision, using a single 10 mm trochar through which a 10 mm laparoscope is inserted. This laparoscope has a single 5 mm operating channel through which the various long operative hand instruments are passed to perform the laparoscopic procedure. We have been able to effectively use the STILS procedure for various gynecological procedures such as hysterectomy and bilateral salpingo-oophorectomy with bowel adhesiolysis. The use of only one intraumbilical 10mm incision offers all the benefits of minimally invasive surgery like minimal bleeding, less post operative pain, short hospital stay, early return to daily activity, less chance of wound infection and port site hernia, and a virtually invisible cosmetic scar.
Case presentation
Investigations
Following evidence of a bulky uterus with an intramural fibroid at pelvic ultrasonography and histological findings of a non-malignant, secretory endometrium in a preoperative endometrial biopsy, the patient, a 43- year old lady , para two, with two previous normal vaginal deliveries, with severe menorrhagia and dysmenorrhea since one year, was counseled to undergo a laparoscopic hysterectomy. . After adequate preoperative bowel preparation, she was taken up for a single 10 mm trochar-incision laparoscopic hysterectomy.
Instruments
14 F Foley’s Catheter, Linen sutures for cervical traction,Tenaculum, Tintara uterine manipulator, No.11 stab knife, Verres needle, 10 mm Trocar , 10 mm 0 degree Operating Laparoscope 26.5 cm length and wide angle view with a 5 mm operating channel, A single chip CCD Camera, Bipolar Generator 50 Watts.,Long 43 cm operating instruments :
5 mm Bipolar Graspe ,5 mm Curved Metzenbaum Scissors, 5 mm Monopolar hook electrode, Suction Irrigation Cannula ,Vaginal Tube / Colpotomiser .
Procedure
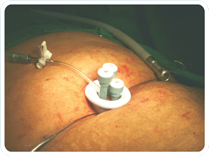
Following adequate bowel preparation, the patient was administered general anesthesia (GA), placed in an extended lithotomy position and a 14 F Foley’s Catheter placed to drain the urinary bladder intraoperatively. Cervical traction suture was placed with linen sutures. Subsequently, the cervix was held with a tenaculum and a uterine manipulator was introduced. A 10mm intraumbilical vertical incision was made with a No.11 stab knife, the Verres needle introduced and its position checked by the hanging drop method. A pneumoperitoneum was created using CO2 at a pressure of 15 mm of Hg, the 10 mm Trocar with a side stop cock for connecting the CO2 tubing is inserted and the 10 mm 0 degree Operating Laparoscope with a 5 mm operating channel introduced. A single chip CCD Camera was used to perform the surgery.
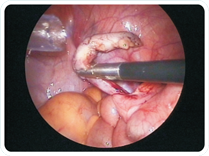
Long 43 cm standard laparoscopic instruments ( 5 mm bipolar grasper, 5 mm scissors, monopolar hook electrode, suction irrigation cannula and vaginal tube/colpotomiser) were used to perform the surgery. The correct presentation of the target organ and tissues was facilitated with the help of an intra-uterine manipulator. As there is no additional side port or instrument, the need for optimum manipulation of the uterus needs to be emphasized .The abdominal and pelvis organs were inspected and since the tubes and ovaries were normal, a decision was taken to retain them.
The cornual structures (round ligament, Fallopian tube and ovarian ligaments) were bipolar coagulated and cut on either sides. The uterovesical fold of peritoneum was incised and pushed inferiorly along with the bladder .The posterior leaf of the broad ligament was dissected and cut upto the insertion of the uterosacral ligaments.
The uterine pedicle was skeletonized and the bladder pushed inferiorly upto the paracolpos so as to keep the ureter away at the time of coagulating the uterine pedicles. Bipolar coagulation of the ascending uterine vessels was performed followed by the main uterine pedicle. After this, the pedicle was cut on either side.
The descending uterine vessels and the cervicovaginal branch of the descending uterine artery was carefully coagulated and cut. This meticulous dissection helps to delineate the cervix and upper vagina at the lateral fornices. The vaginal tube/colpotomiser (with a moist pack placed within it to prevent loss of pneumoperitoneum) was placed to delineate the vaginal fornices. Superior pushing of the tube by the assistant at the vaginal end of the patient was done simultaneously with traction onto the stay sutures over the cervix to make the vaginal fornices prominent. Circumferential colpotomy was done using a monopolar hook electrode thus seperating the uterus and cervix from the vagina without cutting the uterosacral ligaments which are attached to the lower cervix and vault of the vagina.
The vaginal tube was withdrawn and the uterus and cervix extracted vaginally. The vagina was closed with 1 no Vicryl suture ( placed in a continuous locking fashion, taking special care to include the uterosacral ligaments along with the vaginal angles at the lateral fornix.
The laparoscope was reintroduced and the pelvis irrigated with 0.9% normal saline using a suction irrigation cannula. Complete hemostasis was checked for and the laparoscope withdrawn. The 10 mm trochar removed, the fascia closed with 1-0 Vicryl, and 2-0 Monocryl suture placed subcuticularly to close the 10 mm wound. The total operating time was 75 minutes and the blood loss was less than 25 mL. The Foley’s catheter was removed immediately after the surgery. The patient had an excellent post operative recovery and was sitting in bed with minimal discomfort 4 hours after the surgery and was able to mobilize herself and go to the washroom to pass urine without assistance. A liquid diet was started 6 hours post operatively and she was discharged from the hospital in less than 24 hours. Oral antibiotics were prescribed for 5 days.
Result
The specimen was sent for histopathology and it revealed a fibroid uterus and adenomyosis. The cervix revealed no abnormality. The patient’s recovery was uneventful with minimal to no pain and she was fit to resume her daily activities in a week’s time. The scar healed with an excellent cosmetic result.A total number of 30 Laparoscopic Hysterectomies have been performed by us till date using the single trochar incision technique(STILS).In two of these cases a bilateral salpingo oophorectomy was also performed.One case involved omental and small bowel adhesiolysis.
Discussion
Single-incision laparoscopic surgery is a rapidly evolving field as a bridge between traditional laparoscopic surgery and natural orifice transluminal endoscopic surgery.4However, though single incisions, and particularly the umbilicus, have been used for the manifold advantages they offer, either more than one port has frequently been used or more than one operating channel where single-port surgeries were performed.SILS is a burgeoning technical advance whose advantages in terms of reduced pain, faster recovery and reduced convalescence are by no means established. The issues like post operative wound complications like seroma formation and port site herniation have been completely settled by the use of our technique of using a single 10-mm incision in the STILS technique. Recently, exceedingly small single port devices have been explored in gynaecology. Chong et al . reported on a series of 61 patients using a 2-mm miniport with standard trocar and instrumentation for the treatment of benign gynaecological disease.The result demonstrated that a 2-mm miniport is safe and feasible to use, and patient satisfaction was high, as greater than 80% of patients were satisfied with their surgical experience and 94% were satisfied with cosmetic results.(5)
Table 1. Advantages and limitations of STILS laparoscopy
Advantages
1. minimal bleeding
2. less post operative pain (only one 10 mm intraumbilical incision)
3. short hospital stay ,
4. early mobilization and return to daily activity,
5. less chance of wound infection and port site hernia,
6. excellent cosmetic scar which is virtually invisible,
7. Reduced/lack of dependence on the assistant. |
Limitations
1. The requirement of a special operating channel laparoscope and long instruments.
2. The surgeon has to adapt to the co axial and simultaneous movement of the telescope and the operating instruments.
3. The larger size of the uterus may be difficult to manage and may need traction or retraction to expose the target tissues, which can be offered in the SILS technique or by standard laparoscopy.
4. The vagina can only be sutured by the vaginal route. |
However, most of these limitations are subjective to the skill and experience of the surgeon, who with progressive practice and a little more perseverance can do seemingly impossible instrument maneuvers with ease. A careful selection of cases and technique will help the surgeon to offer progressive levels of minimally invasive surgery, ranging from (1) standard laparoscopic hysterectomy - where 4 incisions ( 10 mm x 1 mm intraumbilical incision and 5 mm x 3 incisions) are made over the anterior abdominal wall, to (2) SILS hysterectomy - where a 2.5 cm umbilical incision is made into which special port having channels for 3 trochars are introduced, to (3) STILS hysterectomy – where only one 10 mm incision is made through which the Operating Laparoscope is passed.This technique is definitely the least invasive, doing away with the 3 x 5 mm incisions or the 2 – 2.5 cm incision of the SILS Hysterectomy and the use of an expensive special port. The operating laparoscope used in the STILS Technique offers a distinct advantage over the SILS technique because the camera as well as the operating instrument is in the hands of the operating surgeon and thus the difficulty of correct endoscopic view and dependency on the assistant surgeon who holds the camera is eliminated. Even lateral areas can be accessed and the surgeon can work in a limited space very safely. Hand eye coordination is improved tremendously as the camera and the operating instrument is working in unision.
The importance of the vaginal manipulation needs to be specifically addressed. Since there are no additional instruments for retraction, it is only the manipulator which will help in the correct presentation of the organ and target tissues. It must be noted that if at the time of initial inspection of the pelvic organs, the surgeon finds that the case is moderately difficult ,that ancillary instruments will be needed then the SILS technique can be adopted. In even more difficult cases, the operating telescope can be removed, replaced with a 10 mm 0 or 30 degree telescope through the same intraumbilical trochar and 2 or 3 side trochars can be introduced and the standard laparoscopic surgery can be performed.In our series of 20 cases of laparoscopic hysterectomies the surgery was completed through only one 10 mm trochar and no additional trochars or port were introduced.
Conclusion
This novel laparoscopic technique improvised by us ( STILS laparoscopic Surgery) is simple to perform, easily reproducible ,that can be performed with standard laparoscopic instruments and with many advantages as mentioned above. It offers an excellent alternative to the conventional multi-port, multichannel invasive surgery in carefully selected patients,This technique enables the laparoscopic surgeon to perform major surgeries like hysterectomy, bilateral salpingo-oophorectomy and bowel adhesiolysis, with all the benefits of standard laparoscopic surgery and minimal invasive surgery. By employing a only a single operating channel, this technique helps to reduce the complications of multiple ports as in Standard Laparoscopic Surgery or that of large incision and port of SILS Technique. Thus making key hole surgery a practical reality thereby offering the patient minimally invasive surgery in the true sense.
|